Center for Assistive Technology and Environmental Access
Georgia Institute of Technology
ABSTRACT
The alleviation pressure (AP) cushion is a dynamic cushion system with three bladders at the pelvic region. The bladders can be deflated and inflated in a certain sequence to relieve the pressure on the ischial tuberosities (IT) and coccyx/sacrum. The design of the foam base, bladder and pneumatic and electronic system of the AP cushion is discussed in this paper. And testing is conducted to verify the effectiveness of the AP cushion.
Keywords:
cushion; bladder; pressure ulcer
INTRODUCTION
 Figure 1 AP cushion: Off-loading at the ischial tuberosities (left) Off-loading at the coccyx/sacrum
Figure 1 AP cushion: Off-loading at the ischial tuberosities (left) Off-loading at the coccyx/sacrum A pressure ulcer is an area of damaged skin and tissue caused by sustained pressure induced to the supporting surface of the body weight[1]. The Agency for Health Care Policy and Research (now AHRQ) estimate that 1 to 3 million adults have pressure ulcers. Pressure ulcers are extremely costly, in both fiscal and clinical terms. with an average cost range of $500 to $40,000 to treat and heal each ulcer. Associated health costs related to treating pressure ulcers exceeds $8 billion annually. Pressure ulcers have been identified as 3 public health concern by the federal government within the Healthy People 2010 initiative and the National Quality Forum.
The AP cushion is a self-contained dynamic off-loading wheelchair cushion, designed to alleviate pressure under the primary at-risk sites for the seated individual: the ischial tuberosities (IT) and coccyx/sacrum. It has three bladders at the pelvic region that are deflated and passively inflated in a pre-defined sequence. The coordinated sequence of deflation/inflation of the bladders serves as an intermittent pressure relief, and thus can aid in healing pressure ulcers or help reduce the risk of pressure ulcer caused by prolonged sitting. Further, the cushion uses programmable electronics which allows customization of a pressure relief schedule. The clinician can easily program (via a PC) different modes of operation –sequence and timing of the bladder deflation/inflation cycles– to best suit a client’s needs. Sale of such a cushion would be to individuals, as well as to health care facilities with a focus in wound healing. This cushion could be an integral component of acute rehabilitation status post pressure ulcer surgery. The target end user population consists of any wheelchair user with a current pressure ulcer or at high risk of pressure ulcer development due to impaired mobility and sensation, especially those with history of a pressure ulcer or ulcers.
MATERIAL & DESIGN
The foam base has the pelvic contour based on anthropometry to ensure good postural support and pressure distribution. The contour is designed to be scalable in size to accommodate larger and smaller size cushions. A cavity for the electronics is carved into the front section of the cushion. Space for the bladders is cut from the pelvic well, oversized by ~.5cm on all sides to limit interference with the foam base as the bladders deflate.
Data Taken |
Time |
Bladder Action |
|---|---|---|
Full Inflation Pre |
0:00 |
Before power on, 1 min after sitting |
|
0:25 |
ITs fully deflated |
IT deflate 1 |
0:45 |
Midpoint of IT deflation |
|
1:10 |
ITs released |
|
1:55 |
Sacrum deflation begins |
|
2:20 |
Sacrum fully deflated |
Sacral deflate 1 |
2:40 |
Midpoint of sacral deflation |
|
3:05 |
Sacrum released |
|
3:50 |
(cycle 2) ITs full deflated |
IT deflate 2 |
4:35 |
Midpoint of IT deflation |
|
5:00 |
ITs released |
|
5:45 |
Sacrum deflation begins |
|
6:10 |
Sacrum full deflated |
Sacral deflate 2 |
6:30 |
Midpoint of sacral deflation |
|
6:55 |
Sacrum released. Turn power off. |
Full Inflate Post 1 ( 1min) |
7:55 |
1 minute after deflation cycles completed |
Full Inflate Post 2 (6 min) |
12:55 |
6 minutes after deflation cycles completed |
The bladders are constructed from block of PU foam, with a rigid plastic base, and thermo-formed PU shell. The initial bladder designs had problems with a consistent flat top surface in the deflated state. The center of the bladder would deform quicker/greater than the edges, resulting in “cupping” of the surface and pressure points at the corners. The “flatness” of the surface is controlled by two design features—channels and contours. A rigid base was created with crisscrossing channels recessed into the surface leading from the valve located at the center, to perforations along the edge. This base design directs airflow to the edges of the bladder, encouraging the edges to compress at the same rate as the center, resulting in a flat surface as the bladder deflates. The foam within the bladder was given a saw-tooth profile of evenly spaced vertical/diagonal/horizontal cuts (effectively reducing surface tension) to encourage the edges to compress at the same rate as the center.
The AP cushion control system is a combination of pneumatic and electronic systems. The main controller is a PIC16F877A microprocessor from Microchips. The cushion can be set into different modes by a simple switch. Both the time parameters and the bladder motion mode are programmable via a USB/serial cable and a connected PC with the AP Cushion software installed. Each bladder is connected with two valves, one connects to the pump and the other connects to the air drain. By opening and closing the valves, the bladder is able to deflate, hold or inflate. In order to save power, we use the Normally Open connectors on the L valves and the Normally Closed connectors on the S valves. In this way, when there is no electricity, the bladders will be in release state. The occupancy switch is designed to detect whether a user is sitting on the cushion. The switch connects to the microcontroller. A low voltage indicates there is user seated on the cushion. The cushion will turn off again automatically after detection of 5 minutes continuous vacancy. A 1500mAh lithium ion rechargeable battery is used to ensure that the cushion will operate for up to 16 hours.
TESTING RESULTS
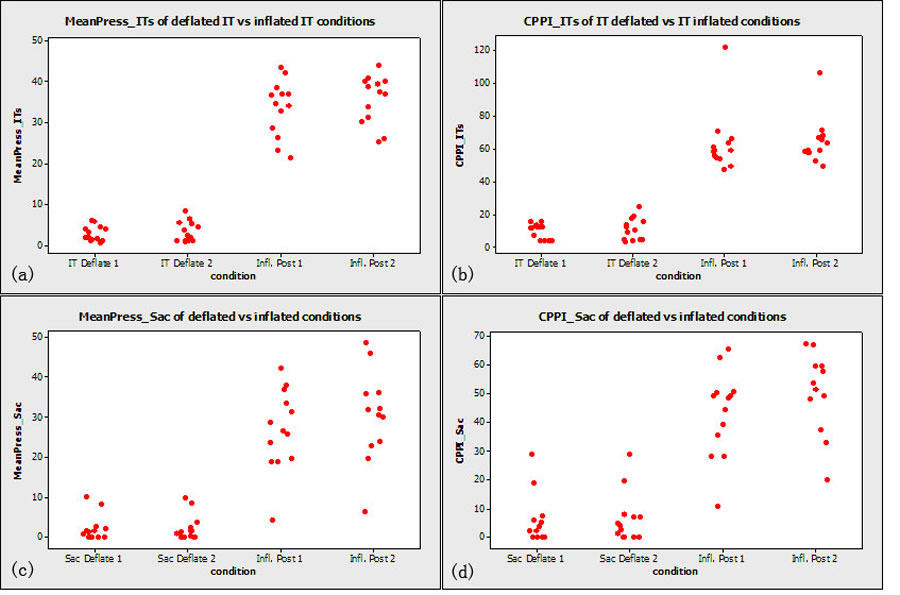 Two variables were chosen to reflect effectiveness of off-loading: mean pressure and Peak Pressure Index (PPI). Both variables were calculated within the bladder areas of interest, either the sacral or IT. While mean pressure reflects loading over the entire bladder area, PPI focuses on the maximum pressure, which is generally associated with a bony prominence. PPI is defined as the highest recorded average pressure value within a 9-10cm2 area (the approximate contact area of an IT or other bony prominence). Figure 3 shows the pressure comparisons between bladders deflated state and inflated state.
Two variables were chosen to reflect effectiveness of off-loading: mean pressure and Peak Pressure Index (PPI). Both variables were calculated within the bladder areas of interest, either the sacral or IT. While mean pressure reflects loading over the entire bladder area, PPI focuses on the maximum pressure, which is generally associated with a bony prominence. PPI is defined as the highest recorded average pressure value within a 9-10cm2 area (the approximate contact area of an IT or other bony prominence). Figure 3 shows the pressure comparisons between bladders deflated state and inflated state. The dynamic bladder sequence utilized was simultaneous deflation and re-inflation of the two ischial tuberosity bladders, followed by deflation and re-inflation of the sacral bladder. Cushion settings were as follows: 25 seconds deflation time, 45 seconds held deflated, 45 seconds between IT and sacrum bladder deflations, and 45 seconds between full cycles. The left column in table 1 lists the seven points where frames of data were collected. Three frames were collected in a five second period for each point. The three frames were then averaged for analysis. 14 Adult wheelchair users with spinal cord injury enrolled in the study.
Results of the testing showed that the AP Cushion effectively off-loaded the bony prominences with bladder deflation. Moreover, interface pressures measured during the inflated states reflected effective pressure distribution. This highlights the effectiveness of the design with respect to the static components: pelvic contour, foam base material and height, as well as bladder material, size and location. This test series represented only a short term trial of the cushion. Each subject sat for two 13 minute bouts. Thus possible changes in interface pressure for long duration sitting are not yet known. This requires further testing.
REFERENCES
- Ambung SR, Miller WL, Bosley LM. The 1999 national pressure ulcer prevalence survey: a benchmarking approach. Adv Skin and Wound Care. 2001;Nov/Dec (14):297-301.
- Fuhrer M, Garber S, Rintola D, Clearman R, Hart K. Pressure ulcers in community-resident persons with spinal cord injury: prevalence and risk factors. Archives of Physical Medicine and Rehabilitation. 1993;74(11):1172-7.
- Lyder C, Preston J, Scinto J, Grady J, Ahearn D. Medicare quality indicator system: pressure ulcer prediction and prevention module: final report: US Healthcare Financing Administration; 1998.
Linhua Kong
Phone: 404 385 4691
490 Tenth Street
Atlanta, Georgia 30318
Word Version PDF Version